2022 FSA Podium and Poster Abstracts
P059: IMPROVEMENT IN POSTOPERATIVE CARE OF INTRAOPERATIVE RECALL
Muna Oli, MD; Hope Sprunger, MD; Lawrence Caruso, MD; Nik Gravenstein, MD; Stephanie Gore, MSN, RN, CCRNK; University of Florida Shands Hospital
Introduction/Background: Intraoperative recall is reported as occurring in 0.1%-0.2% of high risk surgeries. Intra-op recall can cause patient as well as provider psychological distress.The purpose of this quality improvement project is to develop and implement an evidence-based protocol to guide treatment of intra-op recall immediately after surgery and onward. This project has four stages.
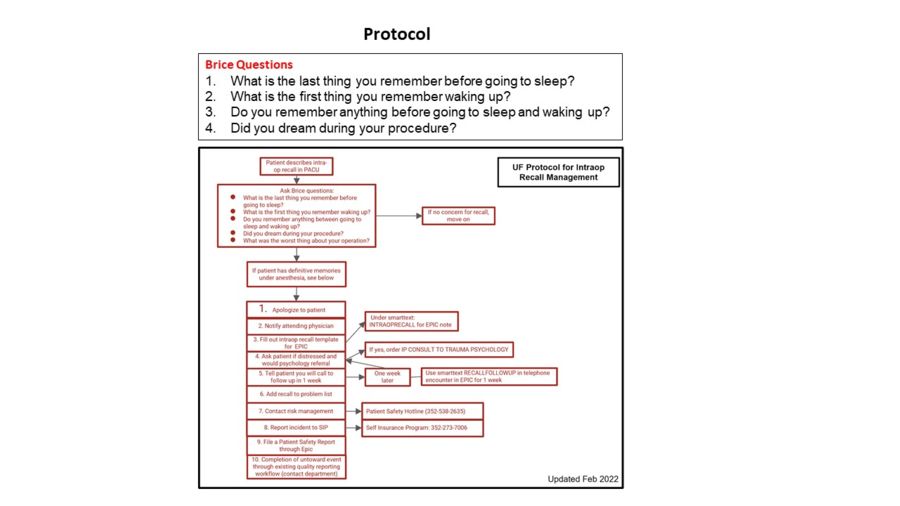
Methods: The project includes four phases: pre-assessment, protocol creation, education and implementation, then post-assessment. The initial pre-assessment established a base knowledge and survey of experience with recall within the UF anesthesia staff. The protocol was developed using literature and expert guidance. The protocol includes communication with patient day of recall and one week post-op follow up, offering a psychological consult, and documentation. Education of how to evaluate and document intra-op recall for anesthesia providers will be performed via email and shared department drive for easy access. Pre and post-assessment of knowledge and confidence in management will be performed via email survey.
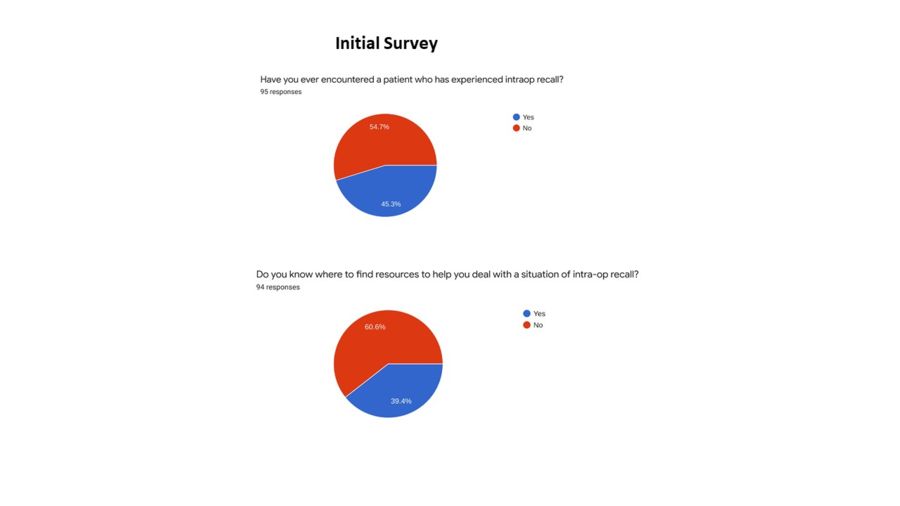
Results: For phase 1 of this project, the results indicated a lack of education on how to identify and handle an incident of intra-op recall. Of the surveyed staff, 46% lacked confidence in how they would handle intra-op recall. Staff brought up valid points regarding clarifying patient expectations between Monitored Anesthesia Care (MAC) and General Anesthesia (GA). Below are some of the results from our pre-assessment.
Our team developed a protocol including use of Brice questions that is now available for our department in the shared drive. We are in the process of collecting data from our post-survey. We anticipate increased confidence in follow up care for intra-op recall.
Discussion/Conclusion: The ultimate goal of assessing, educating, and creating resources for care of intraoperative recall was to improve patient care. The pre-assessment noted 45% of clinical staff have cared for patients citing post-operative recall, 60% did not know how to find adequate resources, and 58% desired greater resources for how to care for intra-op recall patients. The protocol designed will allow for treatment of patients and will assist in a more accurate trend of incidence of recall and inciting factors for further improvements. The upcoming steps will include educating our staff on use of protocol and EMR templates for notes on day of incidence and at one week follow up, ordering psychological evaluation and treatment per patient desire, and assessment of pre-op and intra-op factors to recall. The last stage will assess the staff in improvement of understanding and managing of intra-op recall.