2021 FSA Posters
P004: ANESTHETIC CONSIDERATIONS IN A PATIENT WITH LAMELLAR ICHTHYOSIS PRESENTING FOR LUMBAR SURGERY
Kalina Nedeff, MD; Matthew Maggio, MD; Kendall Regional Medical Center
Introduction/Background: Lamellar Ichthyosis (LI) is a rare, inherited disorder of hyperkeratinization. Features of LI pose several anesthetic challenges, of which few reports of anesthetic management have been found.
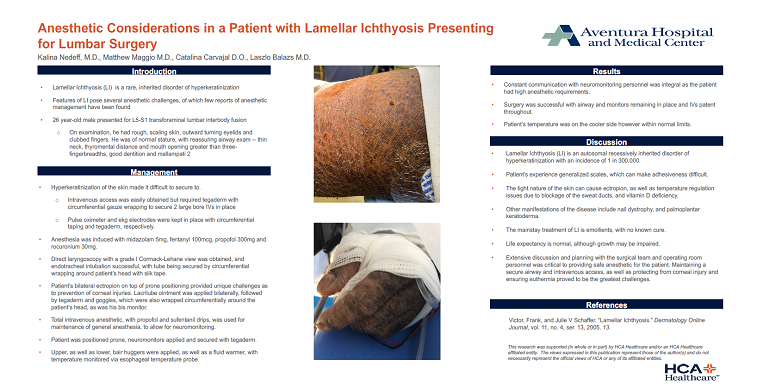
26 year-old male presented for L5-S1 transforaminal lumbar interbody fusion. On examination, he had rough, scaling skin, outward turning eyelids and clubbed fingers. He was of normal stature, with reassuring airway exam -- thin neck, thyromental distance and mouth opening greater than three-fingerbreadths, good dentition and mallampati 2.
Methods: Patient’s hyperkeratinized skin was difficult to secure to. Intravenous access was easily obtained but required tegaderm with circumferential gauze wrapping to secure 2 large bore IVs in place. Pulse oximeter and ekg electrodes were kept in place with circumferential taping and tegaderm, respectively. Anesthesia was induced with midazolam 5mg, fentanyl 100mcg, propofol 300mg and rocuronium 30mg. Direct laryngoscopy with a grade I Cormack-Lehane view was obtained, and endotracheal intubation successful, with tube being secured by circumferential wrapping around patient’s head with silk tape. Patient’s bilateral ectropion on top of prone positioning provided unique challenges as to prevention of corneal injuries. Lacrilube ointment was applied bilaterally, followed by tegaderm and goggles, which were also wrapped circumferentially around the patient’s head, as was his bis monitor. Total intravenous anesthetic, with propofol and sufentanil drips, was used for maintenance of general anesthesia, to allow for neuromonitoring. Patient was positioned prone, neuromonitors applied and secured with tegaderm and upper, as well as lower, bair huggers applied, as well as a fluid warmer, with temperature monitored via esophageal temperature probe.
Results: Constant communication with neuromonitoring personnel was integral as the patient had high anesthetic requirements. Surgery was successful with airway and monitors remaining in place and IVs patent throughout. Patient’s temperature was on the cooler side however within normal limits.
Discussion/Conclusion: Lamellar Ichthyosis (LI) is an autosomal recessively inherited disorder of hyperkeratinization with an incidence of 1 in 300,000. Patient’s experience generalized scales, which can make adhesiveness difficult. The tight nature of the skin can cause ectropion, as well as temperature regulation issues due to blockage of the sweat ducts, and vitamin D deficiency. Other manifestations of the disease include nail dystrophy, and palmoplantar keratoderma. The mainstay treatment of LI is emollients, with no known cure. Life expectancy is normal, although growth may be impaired. Extensive discussion and planning with the surgical team and operating room personnel was critical to providing safe anesthetic for the patient.
.JPG)