2021 FSA Posters
P003: LARGE TRACHEOESOPHAGEAL FISTULA REPAIR
Lindsey J Laux, MD; Arina Ghosh, MD; Philip Smith, MD; Jackson Memorial Hospital / University of Miami
Background: Tracheoesophageal fistulas (TEFs) are most commonly encountered and discussed in the setting of a congenital abnormality. Less frequently encountered and discussed in anesthesia literature are acquired TEFs and their management. Reported common causes of acquired TEFs include malignancy / radiation, infection, trauma, and prolonged mechanical ventilation. Epidemiologic data regarding this topic is insufficient to estimate the occurrence of acquired TEFs, but TEF definitive repair is always surgical. Depending on the size and location of the fistula, the management of the airway requires thoughtful consideration and planning.
Methods: This case report explores the anesthetic management of a 51yo with a large tracheoesophageal fistula at a large tertiary care center.
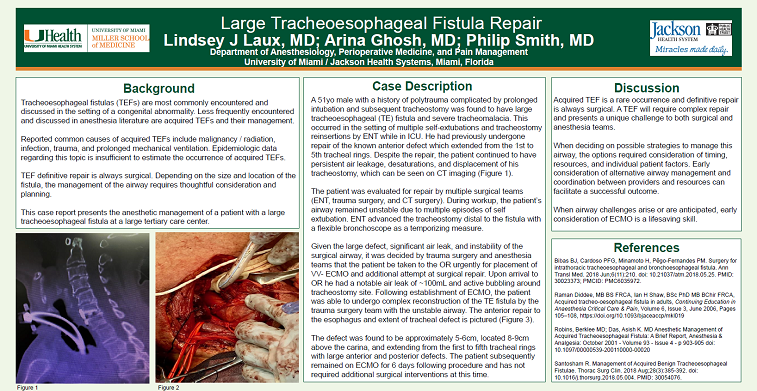
Results: A 51yo male with a history of polytrauma complicated by prolonged intubation and subsequent tracheostomy was found to have large tracheoesophageal (TE) fistula and severe tracheomalacia. This occurred in the setting of multiple self-extubations and tracheostomy reinsertions by ENT while in ICU.
The patient was evaluated for repair by multiple surgical teams (ENT, trauma surgery, and CT surgery). During workup, the patient’s airway remained unstable due to multiple episodes of self extubation. ENT advanced the tracheostomy distal to the fistula with a flexible bronchoscope as a temporizing measure.
Given the large defect, significant air leak, and instability of the surgical airway, it was decided by trauma surgery and anesthesia teams that the patient be taken to the OR urgently for placement of VV- ECMO and repair. Following establishment of ECMO, the patient was able to undergo complex reconstruction of the TE fistula by the trauma surgery team. The patient subsequently remained on ECMO for 6 days following procedure and has not required additional surgical interventions at this time.
Discussion: Acquired TEF is a rare occurrence and definitive repair is surgical. A TEF will require complex repair and presents a unique challenge to both surgical and anesthesia teams. When deciding on possible strategies to manage this airway, the options required consideration of timing, resources, and individual patient factors. Early consideration of alternative airway management and coordination between providers and resources can facilitate a successful outcome. When airway challenges arise or are anticipated, early consideration of ECMO is a lifesaving skill.